Become an Authorized Carrier of Truehope Products
A variety of health care professionals including psychiatrists distribute Truehope products worldwide.
Join an ever growing number of health professionals who connect their patients with Truehope products for balanced mental health and well-being.
For more information or to receive your health professional guide and other educational information please fill out the following form, call 866-397-3795 or fax 866-310-0931.
Physician Support Program
The Truehope Support Program provides support for both users of the nutritional micronutrient treatment, EMPowerplus Advanced, and their doctors. The Truehope Support Program’s goal is to share what we have learned through experience and with the guidance of qualified research advisors, in order that all who choose to use EMPowerplus Advanced may do so safely and as successfully as possible.
We encourage EMPowerplus Advanced users to work closely with their doctors as they progress through the program. We do not seek to replace medical advice nor do we encourage anyone to make a transition to EMPowerplus Advanced on their own. The Truehope Support Program is your professional resource, your access to the latest information and developments on EMPowerplus Advanced, and your link to other doctors who are currently working with EMPowerplus Advanced in their practices.
The Truehope Support Program includes:
- A well-established protocol that you may use and adapt to meet the needs of the individual
- An individualized reporting system for users, in the form of on-line standard psychiatric reporting charts, for you to access and monitor.
- The Truehope Support call center, available free of charge, on an unlimited basis, from 8:00 am to 4:30 pm (Mountain Standard Time), Monday through Friday. The Truehope Support call center is staffed by highly trained, non-medical professionals who are familiar with the use of EMPowerplus Advanced. The call center is available to both you and your patients.
- A website for registered EMPowerplus Advanced users, my.truehope.com, with an online support group message board and more detailed information about the program.
The product, systems, and protocol are the results of university and field research. Each has been designed using our experience and the knowledge of qualified research advisors.
Get More Information
Print Truehope brochures and pamphlets
Download EMPowerplus Advanced™ Informational Pamphlet
Download Truehope Product Guide
We can provide Healthcare Professionals with our EMPowerplus Advanced Professional Guide upon request. This guide will tell you about our protocols and many other important topics. Click here to request your copy.
Reorder Truehope products
You can reorder Truehope products online once you are an authorized carrier. Just go to the Truehope store and sign in with your credentials to receive your exclusive medical professional discounts.
Medical Facts
Research shows it is clear that no one single nutrient (with the exception of lithium) can provide a reliably effective treatment for mood disorders. Rather, the evidence implies that a broad range of nutrients are involved in achieving optimum mental stability:
Various micronutrient-related factors are associated with increased risk of psychiatric illness, and micronutrients play essential roles in an array of brain functions that have been implicated in mood lability. Micronutrient inadequacy may impair one or more of these critical brain functions and result in psychiatric symptoms. The micronutrient-mood regulation mechanisms discussed in this review are not exhaustive, nor are they mutually exclusive; in fact, they may be complementary. For example, neurotransmitter production and regulation, key components of the monoamine or chemical imbalance hypothesis of mood disorders, may work in tandem with neurite outgrowth and gene expression of neurotrophic factors, elements of the network hypothesis; these hypotheses appear to be entirely complementary.28
Intestinal disruption and lack of absorption
Gastrointestinal tract disruption appear to deprive the brain of essential nutrients for key metabolic pathways. Gastrointestinal tract disruptions and psychiatric disorders show remarkably high co-morbidity.29 For example, most studies that have investigated the co-morbidity of irritable bowel syndrome and psychiatric disorders show prevalence of psychiatric disorders in irritable bowel syndrome patients to be 90% or greater.30
Higher, genetically-based micronutrient requirements
Research is uncovering major genetic risk factors in psychiatric illness.31 Up to one-third of gene mutations result in decreased enzyme binding affinity for corresponding coenzymes, including vitamins and minerals.32 As a result, individuals with certain genotypes may have significantly higher requirements for essential micronutrients in key mood-related brain pathways.32 33 44
Low micronutrient intake exacerbates the problem
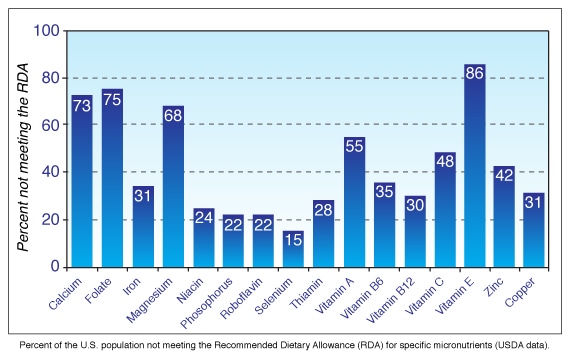
Low micronutrient intake may contribute to psychiatric illness.34 35 36 Intake of many micronutrients is inadequate in the United States, as shown in Figure 2. RDA levels are deemed to be "sufficient to meet the dietary requirements of nearly all (97 to 98 percent) of healthy individuals", but do not ensure mental health for at-risk sub-populations:13 "intake at the level of the RDA or AI would not necessarily be expected to replete individuals previously undernourished, nor would it be adequate for disease states marked by increased requirements."37
Synthesis of neurotransmitters
Many neurotransmitters require micronutrient cofactors in their synthesis. Iron and copper have roles in serotonin and dopamine synthesis.39 40 Folic acid and vitamin B12 are involved as cofactors in serotonin and norepinephrine synthesis.41 Thiamine serves as a coenzyme in acetylcholine, GABA, and glutamate synthesis.42 Vitamin B6 serves as a cofactor in the synthesis of the neurotransmitters dopamine, serotonin, norepinephrine, epinephrine, histamine, and GABA,43 and vitamin B6 deficiency has been shown to reduce brain production of serotonin and GABA.44
Regulation of neurotransmission
Micronutrients play key roles in regulating neuronal transmission. Zinc is extensively involved in synaptic transmission,45 46 both excitatory and inhibitory.47 In certain brain regions, vesicular zinc is co-localized and co-released with glutamate, modulating the function of a number of channels, receptors, and transporters,48 49 including NMDA receptors.50 Magnesium and copper are important modulators of NMDA-receptor activity, which has been implicated in the pathogenesis of mood disorders.51 52
Methylation
Hypomethylation has been reported as a major risk factor for schizophrenia and bipolar disorder.53 Hundreds of methylation reactions occur in the body, including during DNA, RNA, and neurotransmitter synthesis. The neuropsychiatric effects of folate and vitamin B12 deficiencies result from defective methylation processes.54 55 Folate is a precursor to S-adenosyl-L-methionine (SAMe), a methyl donor that has been shown to have antidepressant properties.56 Choline is also major source of methyl groups for methylation reactions,57 and has been reported to enhance symptoms of patients being treated with lithium.58
Prevention of genetic damage
Deficiency of folic acid, niacin, vitamin B6, vitamin B12, vitamin C, vitamin E, iron, or zinc (one or more of which is seen in half the US population59) have been shown to mimic radiation in causing single- and double-strand DNA breaks, which could decrease enzyme affinity for nutrient cofactors.60 61 Folate deficiency of a magnitude seen in 10% of the US population breaks chromosomes by causing massive mis-incorporation of uracil into human DNA.59 In addition, various vitamin and mineral deficiencies have been shown to accelerate mitochondrial decay, leading to DNA damage.62
Gene expression
Various micronutrients are involved in gene expression. Folate plays an essential role in methylation, which is involved in gene expression, transcription, chromatin structure, genomic repair and genomic stability.63 Vitamin A and vitamin E have been reported to have roles in gene expression as well.64 65 Vitamin D, zinc and calcium have been shown to be involved in brain-derived neurotrophic factor (BDNF) gene expression, an effect also seen in clinically effective antidepressants.66 67 68 69 TrkB, a BDNF-activated receptor, has been shown to be activated by zinc and copper.70 71
Neurite outgrowth
Several micronutrients have been shown to be involved in neurite outgrowth, which is critical in optimizing neural networks. Vitamin A is a precursor to retinoic acid, which is extensively involved in neurite outgrowth and axonal elongation.72 73 Calcium plays critical roles in neurite outgrowth.74 75 76 Magnesium, selenium, and copper are also involved.77 78 79
Conclusion
Recent clinical trials using non-lithium micronutrient interventions have shown beneficial effects on mood. Multi-micronutrient interventions appear to be particularly promising. Certain sub-populations may have increased requirements for micronutrients, which are extensively involved in an array of mood-related brain functions. Micronutrient inadequacy may impair one or more critical brain functions, resulting in psychiatric symptoms.
Micronutrient inadequacy impairs mood-related brain function, resulting in psychiatric symptoms. When patients in research samples have multiple micronutrient inadequacies (USDA data38), single-nutrient interventions may show only marginal effects; multiple-nutrient interventions, however, result in more complete, dramatic effects. The concept of multiple-micronutrient inadequacy may explain why clinical trials using single-nutrient interventions show only marginal effects. A broad-spectrum multi-ingredient treatment is required to test the hypothesis that micronutrient inadequacy impairs key brain functions and produces psychiatric symptoms.
Environmental and Genetic Pressures on Brain Functions (PDF)
To understand what makes EMPowerplus™ so effective for bipolar, depression, and other mood disorders, it’s important to recognize the relationship between micronutrient deficiencies and the incidence of mental illness. For example, research on the role of zinc in depression showed that levels of zinc in the blood of depressed subjects was significantly lower than in controls.
Could micronutrient deficiencies be affecting your mental health?
Despite efforts to eat a balanced diet with healthier food choices, this graph from the USDA shows most Americans do not meet the Recommended Daily Allowance (RDA) for many essential micronutrients. This may be one reason why the incidence of mental illness and mood disorders such as bipolar continue to rise at an alarming rate.
The good news? Current research suggests many symptoms of bipolar, depression, anxiety, and ADHD can be reduced or eliminated using the full-spectrum micronutrient formulation of EMPowerplus.
The role of serotonin in mood stability
The “feel good” neurotransmitter serotonin plays a critical role in mood regulation. Most pharmaceutical treatments for depression are known as Selective Serotonin Re-uptake Inhibitors, or SSRIs, and are supposed to keep the mood-balancing effects of serotonin working in the brain longer by blocking its re-absorption in the body.
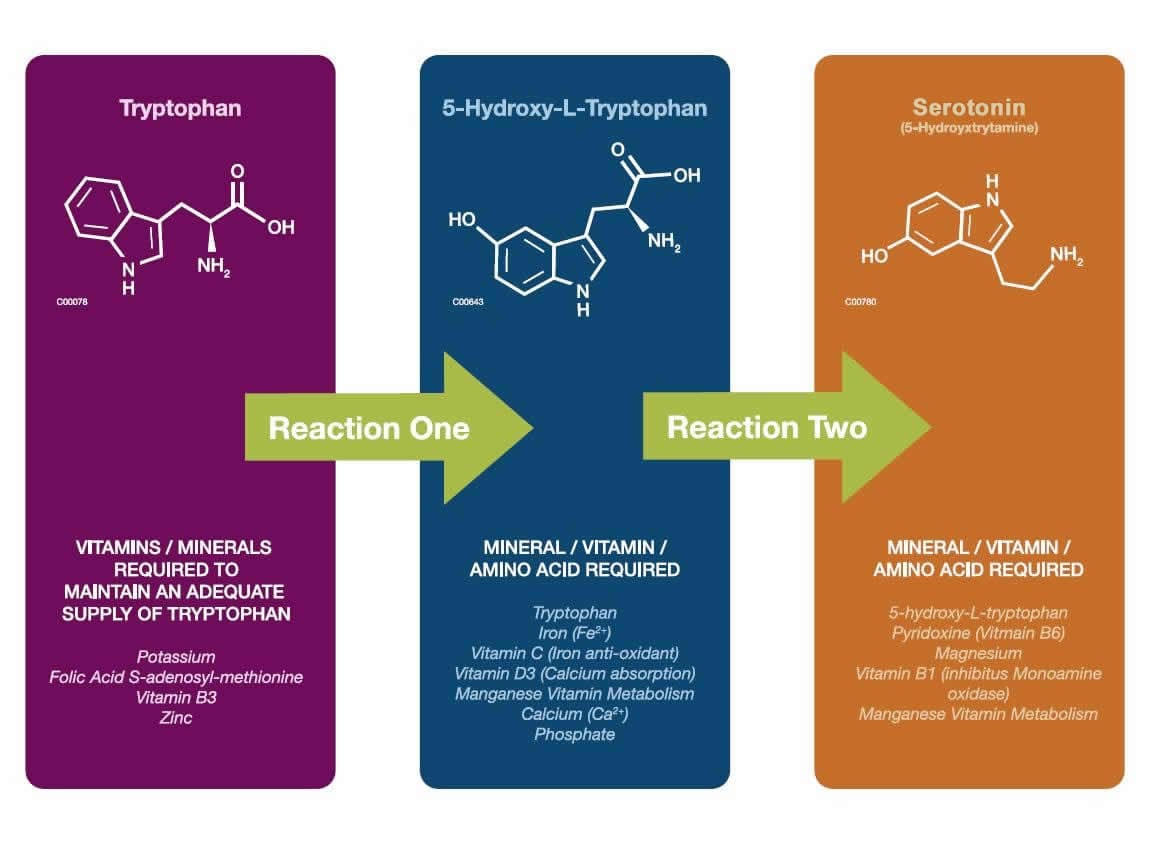
A better way to look at the role of serotonin is to understand how the body creates this essential neurotransmitter. The following diagram details the chemical reactions the body must go through to produce serotonin and demonstrates that:
- Every reaction requires micronutrients to function properly in the production process.
- It is reasonable to assume that dietary deficiencies in micronutrients can slow or even halt the production of serotonin.
- Addressing micronutrient deficiencies with the high quality formula EMPowerplus may give your body what it needs to adequately produce serotonin and other essential neurotransmitters.
The result? Your mood improves and you feel better.
Micronutrient deficiencies can prevent production of other natural chemicals
References
- Freeman MP, Freeman SA. Lithium: clinical considerations in internal medicine. Am J Med. 2006 Jun;119(6):478-81.
- Shiloh R, Weizman A, Weizer N, Dorfman-Etrog P, Munitz H. [Antidepressive effect of pyridoxine (vitamin B6) in neuroleptic-treated schizophrenic patients with co-morbid minor depression--preliminary open-label trial] Harefuah. 2001 May;140(5):369-73, 456.
- Goggans FC. A case of mania secondary to vitamin B12 deficiency. Am J Psychiatry. 1984 Feb;141(2):300-1.
- McLeod MN, Gaynes BN, Golden RN. Chromium potentiation of antidepressant pharmacotherapy for dysthymic disorder in 5 patients. J Clin Psychiatry. 1999 Apr;60(4):237-40.
- McLeod MN, Golden RN. Chromium treatment of depression. Int J Neuropsychopharmacol. 2000 Dec;3(4):311-314.
- Heiden A, Frey R, Presslich O, Blasbichler T, Smetana R, Kasper S. Treatment of severe mania with intravenous magnesium sulphate as a supplementary therapy. Psychiatry Res. 1999 Dec 27;89(3):239-46.
- Chouinard G, Beauclair L, Geiser R, Etienne P. A pilot study of magnesium aspartate hydrochloride (Magnesiocard) as a mood stabilizer for rapid cycling bipolar affective disorder patients. Prog Neuropsychopharmacol Biol Psychiatry. 1990;14(2):171-80.
- Fafouti M, Paparrigopoulos T, Liappas J, Mantouvalos V, Typaldou R, Christodoulou G. Mood disorder with mixed features due to vitamin B(12) and folate deficiency. Gen Hosp Psychiatry. 2002 Mar-Apr;24(2):106-9.
- Walsh W.J., Glab L.B., & Haakenson M.L. (2004) Reduced violent behavior following biochemical therapy. Physiol Behav, 82(5), 835-839.
- Kaplan BJ, Crawford SG, Gardner B, Farrelly G. Treatment of mood lability and explosive rage with minerals and vitamins: two case studies in children. J Child Adolesc Psychopharmacol. 2002 Fall;12(3):205-19.
- Kaplan BJ, Fisher JE, Crawford SG, Field CJ, Kolb B. Improved mood and behavior during treatment with a mineral-vitamin supplement: an open-label case series of children. J Child Adolesc Psychopharmacol. 2004 Spring;14(1):115-22.
- Kaplan BJ, Simpson JS, Ferre RC, Gorman CP, McMullen DM, Crawford SG. Effective mood stabilization with a chelated mineral supplement: an open-label trial in bipolar disorder. J Clin Psychiatry. 2001 Dec;62(12):936-44.
- Popper CW. Do vitamins or minerals (apart from lithium) have mood-stabilizing effects? J Clin Psychiatry. 2001 Dec;62(12):933-5.
- Simmons M. Nutritional approach to bipolar disorder. J Clin Psychiatry. 2003 Mar;64(3):338; author reply 338-9.
- Godfrey PS, Toone BK, Carney MW, Flynn TG, Bottiglieri T, Laundy M, Chanarin I, Reynolds EH. Enhancement of recovery from psychiatric illness by methylfolate. Lancet. 1990 Aug 18;336(8712):392-5.
- Benton, D., Griffiths, R., & Haller, J. (1997). Thiamine supplementation mood and cognitive functioning. Psychopharmacology, 129(1), 66-71.
- Wyatt KM, Dimmock PW, Jones PW, Shaughn O'Brien PM. Efficacy of vitamin B-6 in the treatment of premenstrual syndrome: systematic review. BMJ. 1999 May 22;318(7195):1375-81.
- Thys-Jacobs S, Starkey P, Bernstein D, Tian J. Calcium carbonate and the premenstrual syndrome: effects on premenstrual and menstrual symptoms. Premenstrual Syndrome Study Group. Am J Obstet Gynecol. 1998 Aug;179(2):444-52.
- Davidson JR, Abraham K, Connor KM, McLeod MN. Effectiveness of chromium in atypical depression: a placebo-controlled trial. Biol Psychiatry. 2003 Feb 1;53(3):261-4.
- Giannini AJ, Nakoneczie AM, Melemis SM, Ventresco J, Condon M. Magnesium oxide augmentation of verapamil maintenance therapy in mania. Psychiatry Res. 2000 Feb 14;93(1):83-7.
- Benton D, Cook R. The impact of selenium supplementation on mood. Biol Psychiatry. 1991 Jun 1;29(11):1092-8.
- Cohen BM, Lipinski JF, Altesman RI. Lecithin in the treatment of mania: double-blind, placebo-controlled trials. Am J Psychiatry. 1982 Sep;139(9):1162-4.
- Benton D, Haller J, Fordy J. Vitamin supplementation for 1 year improves mood. Neuropsychobiology. 1995;32(2):98-105.
- Schlebusch L, Bosch BA, Polglase G, Kleinschmidt I, Pillay BJ, Cassimjee MH. A double-blind, placebocontrolled, double-centre study of the effects of an oral multivitamin-mineral combination on stress. S Afr Med J. 2000 Dec;90(12):1216-23.10
- Carroll, D., Ring, C., Suter, M., & Willemsen, G. (2000). The effects of an oral multivitamin combination with calcium, magnesium, and zinc on psychological well-being in healthy young male volunteers: a double-blind placebo-controlled trial. Psychopharmacology (Berl), 150(2), 220-225.
- Schoenthaler SJ, Bier ID. The effect of vitamin-mineral supplementation on juvenile delinquency among American schoolchildren: a randomized, double-blind placebo-controlled trial. J Altern Complement Med. 2000 Feb;6(1):7-17.
- Gesch CB, Hammond SM, Hampson SE, Eves A, Crowder MJ. Influence of supplementary vitamins, minerals and essential fatty acids on the antisocial behaviour of young adult prisoners. Randomised, placebo-controlled trial. Br J Psychiatry. 2002 Jul;181:22-8.
- Castren E. Is mood chemistry? Nat Rev Neurosci. 2005 Mar;6(3):241-6.
- Mayer EA, Craske M, Naliboff BD. Depression, anxiety, and the gastrointestinal system. J Clin Psychiatry. 2001;62 Suppl 8:28-36.
- Whitehead WE, Palsson O, Jones KR. Systematic review of the comorbidity of irritable bowel syndrome with other disorders: what are the causes and implications? Gastroenterology. 2002 Apr;122(4):1140-56.
- Van Den Bogaert A, Del-Favero J, Van Broeckhoven C. Major affective disorders and schizophrenia: a common molecular signature? Hum Mutat. 2006 Sep;27(9):833-53.
- Ames BN, Elson-Schwab I, Silver EA. High-dose vitamin therapy stimulates variant enzymes with decreased coenzyme binding affinity (increased K(m)): relevance to genetic disease and polymorphisms. Am J Clin Nutr. 2002 Apr;75(4):616-58.
- Pauling L. Orthomolecular psychiatry. Varying the concentrations of substances normally present in the human body may control mental disease. Science. 1968 Apr 19;160(825):265-71.
- Liu J, Raine A, Venables PH, Mednick SA. Malnutrition at age 3 years and externalizing behavior problems at ages 8, 11, and 17 years. Am J Psychiatry. 2004 Nov;161(11):2005-13.
- Colton CW, Manderscheid RW. Congruencies in increased mortality rates, years of potential life lost, and causes of death among public mental health clients in eight states. Prev Chronic Dis. 2006 Apr;3(2):A42.
- Sederer LI, Silver L, McVeigh KH, Levy J. Integrating care for medical and mental illnesses. Prev Chronic Dis. 2006 Apr;3(2):A33.
- Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. National Academy Press, Washington, D.C., 1997. Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B-6, Folate, Vitamin B-12, Pantothenic Acid, Biotin, and Choline. National Academy Press, Washington, D.C., 1998.Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids. National Academy Press, Washington, D.C., 2000.Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes: Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. National Academy Press, Washington, D.C., 2001.
- United States Department of Agriculture (USDA) Agriculture Research Service (ARS): Continuing Survey of Food Intakes by Individuals (CSFII): 1994-1996 and 1998 data. Community Nutrition Mapping Project (CNMap) [31 May 2007]. Available from URL: http://www.ars.usda.gov/Services/docs.htm?docid=10709
- Martinez A, Knappskog PM, Haavik J. A structural approach into human tryptophan hydroxylase and its implications for the regulation of serotonin biosynthesis. Curr Med Chem. 2001 Jul;8(9):1077-91.
- Park KH, Lee JR, Hahn HS, Kim YH, Bae CD, Yang JM, Oh S, Bae YJ, Kim DE, Hahn MJ. Inhibitory effect of ammonium tetrathiotungstate on tyrosinase and its kinetic mechanism. Chem Pharm Bull (Tokyo). 2006 Sep;54(9):1266-70.
- Hutto BR. Folate and cobalamin in psychiatric illness. Compr Psychiatry. 1997 Nov-Dec;38(6):305-14.
- Bell IR, Edman JS, Morrow FD, Marby DW, Perrone G, Kayne HL, Greenwald M, Cole JO. Brief communication. Vitamin B1, B2, and B6 augmentation of tricyclic antidepressant treatment in geriatric depression with cognitive dysfunction. J Am Coll Nutr. 1992 Apr;11(2):159-63.
- Baldewicz TT, Goodkin K, Blaney NT, Shor-Posner G, Kumar M, Wilkie FL, Baum MK, Eisdorfer C. Cobalamin level is related to self-reported and clinically rated mood and to syndromal depression in bereaved HIV-1(+) and HIV-1(-) homosexual men. J Psychosom Res. 2000 Feb;48(2):177-85.
- McCarty MF. High-dose pyridoxine as an 'anti-stress' strategy. Med Hypotheses. 2000 May;54(5):803-7.
- Huang EP. Metal ions and synaptic transmission: think zinc. Proc Natl Acad Sci U S A. 1997 Dec 9;94(25):13386-7.11
- Frederickson CJ, Suh SW, Silva D, Frederickson CJ, Thompson RB. Importance of zinc in the central nervous system: the zinc-containing neuron. J Nutr. 2000 May;130(5S Suppl):1471S-83S.
- Cohen-Kfir E, Lee W, Eskandari S, Nelson N. Zinc inhibition of gamma-aminobutyric acid transporter 4 (GAT4) reveals a link between excitatory and inhibitory neurotransmission. Proc Natl Acad Sci U S A. 2005 Apr 26;102(17):6154-9.
- Wall MJ. A role for zinc in cerebellar synaptic transmission? Cerebellum. 2005;4(4):224-9.
- Takeda A. Movement of zinc and its functional significance in the brain. Brain Res Brain Res Rev. 2000 Dec;34(3):137-48.
- Reynolds IJ, Miller RJ. Tricyclic antidepressants block N-methyl-D-aspartate receptors: similarities to the action of zinc. Br J Pharmacol. 1988 Sep;95(1):95-102.
- Siwek M, Wrobel A, Dudek D, Nowak G, Zieba A. [The role of copper and magnesium in the pathogenesis and treatment of affective disorders] Psychiatr Pol. 2005 Sep-Oct;39(5):911-20.
- Schlief ML, Gitlin JD. Copper homeostasis in the CNS: a novel link between the NMDA receptor and copper homeostasis in the hippocampus. Mol Neurobiol. 2006 Apr;33(2):81-90.
- Abdolmaleky HM, Cheng KH, Faraone SV, Wilcox M, Glatt SJ, Gao F, Smith CL, Shafa R, Aeali B, Carnevale J, Pan H, Papageorgis P, Ponte JF, Sivaraman V, Tsuang MT, Thiagalingam S. Hypomethylation of MB-COMT promoter is a major risk factor for schizophrenia and bipolar disorder. Hum Mol Genet. 2006 Nov 1;15(21):3132-45.
- Scott JM, Molloy AM, Kennedy DG, Kennedy S, Weir DG. Effects of the disruption of transmethylation in the central nervous system: an animal model. Acta Neurol Scand Suppl. 1994;154:27-31.
- Bottiglieri T. Folate, vitamin B12, and neuropsychiatric disorders. Nutr Rev. 1996 Dec;54(12):382-90.
- Mischoulon D, Fava M. Role of S-adenosyl-L-methionine in the treatment of depression: a review of the evidence. Am J Clin Nutr. 2002 Nov;76(5):1158S-61S.
- Zeisel SH. Choline: an essential nutrient for humans. Nutrition. 2000 Jul-Aug;16(7-8):669-71.
- Stoll AL, Sachs GS, Cohen BM, Lafer B, Christensen JD, Renshaw PF. Choline in the treatment of rapid-cycling bipolar disorder: clinical and neurochemical findings in lithium-treated patients. Biol Psychiatry. 1996 Sep 1;40(5):382-8.
- Ames BN. A role for supplements in optimizing health: the metabolic tune-up. Arch Biochem Biophys. 2004 Mar 1;423(1):227-34.
- Ames BN. The metabolic tune-up: metabolic harmony and disease prevention. J Nutr. 2003 May;133(5 Suppl 1):1544S-8S.
- Courtemanche C, Huang AC, Elson-Schwab I, Kerry N, Ng BY, Ames BN. Folate deficiency and ionizing radiation cause DNA breaks in primary human lymphocytes: a comparison. FASEB J. 2004 Jan;18(1):209-11.
- Ames BN, Atamna H, Killilea DW. Mineral and vitamin deficiencies can accelerate the mitochondrial decay of aging. Mol Aspects Med. 2005 Aug-Oct;26(4-5):363-78.
- Stanger O. Physiology of folic acid in health and disease. Curr Drug Metab. 2002 Apr;3(2):211-23.
- Ahlemeyer B, Huhne R, Krieglstein J. Retinoic acid potentiated the protective effect of NGF against staurosporine-induced apoptosis in cultured chick neurons by increasing the trkA protein expression. J Neurosci Res. 2000 Jun 15;60(6):767-78.
- Zhang B, Tanaka J, Yang L, Yang L, Sakanaka M, Hata R, Maeda N, Mitsuda N. Protective effect of vitamin E against focal brain ischemia and neuronal death through induction of target genes of hypoxia-inducible factor-1. Neuroscience. 2004;126(2):433-40.
- Nowak G, Legutko B, Szewczyk B, Papp M, Sanak M, Pilc A. Zinc treatment induces cortical brain-derived neurotrophic factor gene expression. Eur J Pharmacol. 2004 May 10;492(1):57-9.
- Mellstrom B, Torres B, Link WA, Naranjo JR. The BDNF gene: exemplifying complexity in Ca2+ -dependent gene expression. Crit Rev Neurobiol. 2004;16(1-2):43-9.
- Finkbeiner S. Calcium regulation of the brain-derived neurotrophic factor gene. Cell Mol Life Sci. 2000 Mar;57(3):394-401.
- Fukuchi M, Tabuchi A, Tsuda M. Transcriptional regulation of neuronal genes and its effect on neural functions: cumulative mRNA expression of PACAP and BDNF genes controlled by calcium and cAMP signals in neurons. J Pharmacol Sci. 2005 Jul;98(3):212-8.
- Hwang JJ, Park MH, Choi SY, Koh JY. Activation of the Trk signaling pathway by extracellular zinc. Role of metalloproteinases. J Biol Chem. 2005 Mar 25;280(12):11995-2001.
- Hwang JJ, Park MH, Koh JY. Copper activates TrkB in cortical neurons in a metalloproteinase-dependent manner. J Neurosci Res. 2007 May 22.12
- Clagett-Dame M, McNeill EM, Muley PD. Role of all-trans retinoic acid in neurite outgrowth and axonal elongation. J Neurobiol. 2006 Jun;66(7):739-56.
- So PL, Yip PK, Bunting S, Wong LF, Mazarakis ND, Hall S, McMahon S, Maden M, Corcoran JP. Interactions between retinoic acid, nerve growth factor and sonic hedgehog signalling pathways in neurite outgrowth. Dev Biol. 2006 Oct 1;298(1):167-75.
- Mikoshiba K, Fukuda M, Ibata K, Kabayama H, Mizutani A. Role of synaptotagmin, a Ca2+ and inositol polyphosphate binding protein, in neurotransmitter release and neurite outgrowth. Chem Phys Lipids. 1999 Apr;98(1-2):59-67.
- Lautermilch NJ, Spitzer NC. Regulation of calcineurin by growth cone calcium waves controls neurite extension. J Neurosci. 2000 Jan 1;20(1):315-25.
- Dijkhuizen PA, Ghosh A. Regulation of dendritic growth by calcium and neurotrophin signaling. Prog Brain Res. 2005;147:17-27.
- Koike T. Nerve growth factor-induced neurite outgrowth of rat pheochromocytoma PC 12 cells: dependence on extracellular Mg2+ and Ca2+. Brain Res. 1983 Dec 19;289(1-2):293-303.
- Miyaguchi K. Localization of selenium-binding protein at the tips of rapidly extending protrusions. Histochem Cell Biol. 2004 May;121(5):371-6.
- Birkaya B, Aletta JM. NGF promotes copper accumulation required for optimum neurite outgrowth and protein methylation. J Neurobiol. 2005 Apr;63(1):49-61.